What is infertility?
Infertility is a multifactorial and complex condition that affects approximately 15% of couples of reproductive age. It can be defined as the inability to achieve or complete a pregnancy after a period of one year of sexual intercourse without contraception and is often attributed to men and women alike.
What types of infertility are there?
As mentioned, there are multiple causes to explain the origin of infertility and there are several types of classification depending on the approach to these causes.
Primary and secondary infertility
- Primary infertility: When the couple has not achieved pregnancy or has achieved a gestation that has not reached full term with a live newborn.
- Secondary infertility: when after having one or more children, the couple does not achieve a new full-term pregnancy with a live newborn.
The different infertility problems can also be classified on the basis of the following criteria:
- Defective gamete production: The problems that will lead to infertility can originate in any of the phases of spermatogenesis (formation of spermatozoa) and ovogenesis (formation of eggs).
- Obstruction of the reproductive tract
- Inflammation or immune dysfunction
- Sexual disturbances
How does fertility vary with age?
- 20 to 25 years: About 25%
- 25 to 30 years: About 20%
- 30 to 35 years: About 15%
- 35 to 40 years old: About 10%
- 40 years old: Around 5%
- Over 40 years old: Around 1%

What are the genetic causes of infertility?
In couples who are unable to have children, one of the main genetic causes of infertility are chromosomal alterations, whether numerical or structural. In addition to these chromosomal alterations, genetic changes are sometimes detected at the DNA level (mutations in certain genes). In all cases, specific genetic testing may be necessary to identify the cause.
Chromosomal abnormalities
Chromosomal abnormalities are relatively common in humans and are among the most frequent genetic causes of:
- Infertility: as they prevent the correct development of sperm and eggs.
- Recurrent miscarriages: these genetic defects prevent carrier embryos from developing normally, so that a miscarriage usually occurs before 12 weeks of pregnancy.
- Birth of affected offspring: in cases where, despite these genetic defects, the pregnancy is carried to term, the offspring often have physical and intellectual problems.
In infertile men, the frequency of these somatic chromosomal abnormalities varies from 3% in cases of mild fertility impairment to 19% in cases of non-obstructive azoospermia. Chromosomal abnormalities are divided into numerical and structural:
Numerical abnormalities (Aneuplodies)
Humans have 46 chromosomes in each cell of the body. Numerical chromosomal abnormalities are the loss or gain of one or more chromosomes.
Regarding numerical abnormalities and their relation to infertility:
- Males with a karyotype 47, XXY or Klinefelter syndrome represent the most frequent aneuploidy in infertile male patients, with an incidence of 0.3%, which is 3-5 times higher than that described in the general population.
- Females with a karyotype 45, X0 or Turner syndrome.
- Chromosomal abnormalities can also appear as an error during the formation of the oocyte or spermatozoon in the process known as meiosis. As a result, when fertilisation occurs, the embryo will have the wrong (too many or too few) chromosomes. This error can cause miscarriages or result in individuals with various conditions (often mental retardation).
Structural abnormalities
In the case of structural abnormalities, the number of chromosomes is correct but not their structure. Among the structural anomalies we distinguish:
- Those consisting of a gain (duplication, insertion) or loss (deletion) of genetic material. This type of anomaly usually has a phenotypic implication for the carrier.
- Those in which there is no gain or loss of material but only a rearrangement (Robertsonian translocations, reciprocal translocations and inversions). These abnormalities usually have no consequences for the carrier, although they may affect the reproductive process. These abnormalities hinder the formation of eggs and sperm, which increases the risk of miscarriages or affected offspring.
What are the most common genetic causes of male infertility?
- Klinefelter’s syndrome: As mentioned above, these are males with an extra X chromosome (47, XXY). There are also cases of 48, XXXY, and 49,XXXXY.
After birth and during childhood, these children usually develop normally. Upon reaching adulthood, men with Klinefelter syndrome are unable to procreate, due to a complete absence of sperm in the ejaculate, known as azoospermia. - Microdeletions on the Y chromosome: The Y chromosome contains genes essential for spermatogenesis and proper development of the male gonads. Microdeletions on the Y chromosome are the leading genetic cause of infertility, with a prevalence of 10-15% in cases of non-obstructive azoospermia and 5-10% in cases of severe oligospermia. Depending on the region affected, AZFa, AZFb or AZFc, the alteration of sperm development is different. Genetic analysis allows these deletions to be detected.
- Sperm DNA fragmentation: These are breaks in the genetic material of spermatozoa, which have been associated with a reduction in fertilisation and pregnancy rates, low embryo quality and an increase in miscarriage rates.
- Most frequent mutations: Among the most frequent mutations are those affecting the CFTR and AR genes.
Mutations in the CTFR gene are responsible for cystic fibrosis, and one of its manifestations is the absence of vas deferens in the testicles. Between 60% and 90% of infertile patients with absent vas deferens are carriers of this mutation. Cystic fibrosis is inherited in an autosomal recessive manner and the probability of being a healthy carrier of a mutation leading to cystic fibrosis is relatively high: 1 in 25 people is a carrier. Therefore, if the male has an absence of vas deferens, offspring obtained through assisted fertilisation have an increased risk of developing cystic fibrosis. In these cases, it is advised that the female partner also undergoes genetic testing for the CFTR gene to exclude the possibility that she also has a recessive predisposition which, together with the recessive predisposition of the male partner, may lead to disease in their common child.
Mutations in the AR gene, located on the X chromosome, cause a variety of defects collectively known as androgen insensitivity syndrome. Mutations in AR cause azoospermia and affect 2% of the infertile patient population. - Other mutations affecting fertility in men: In recent years, mutations have been detected in several genes that are also associated with certain cases of infertility. These genes include TEX11, AURKC, SYCP3, DNAH1, ZPBP, SYCE1, CATSPER1, or NR5A1, among others.
What are the most common genetic causes of female infertility?
- Turner syndrome: As explained above, Turner syndrome occurs when one of the two sex chromosomes (XX) is missing in the nucleus of all or part of the cells (mosaic type) of a female. Women with this syndrome usually have short stature, nuchal folding, occasional malformations of internal organs, lack of development of secondary sexual characteristics and are therefore infertile.
- Mutations in the FMR1 gene: Women with premature ovarian failure may carry a so-called premutation in the Fragile X gene (FMR1 gene). In addition, they have a significantly increased risk of having a child with intellectual disability due to Fragile X Syndrome.
- Triple X syndrome: Also called trisomy X or 47,XXX, this is a genetic disorder that affects approximately 1 in 1,000 women. Many girls and women with triple X syndrome have no symptoms or only mild symptoms. In other cases, symptoms may be more marked and possibly include developmental delays and learning difficulties. On the fertility side, premature ovarian failure has also been reported in triple X syndrome.
- FSH receptor mutations: These may also be associated with premature ovarian failure.
- Thrombophilias
What are the most common genetic causes of recurrent miscarriages?
More than half of all miscarriages are due to chromosomal abnormalities in embryos. In most cases, these abnormalities are the accidental result of the complex processes surrounding the reproductive process (from egg and sperm formation to the early stages of embryo development).
However, in about five percent of couples with recurrent miscarriages, it is an inherited disorder usually due to structural chromosomal abnormalities. The carrier of this genetic abnormality is physically and mentally healthy. However, during the formation of the reproductive cells (sperm or egg cells) and the subsequent fertilisation, incorrect combinations can occur, resulting in the subsequent death of the embryo or abnormal development of the child.
There are also other causes of miscarriages, such as blood clotting disorders (thrombophilia), organic causes (congenital malformations of the uterus, fibroids, etc.) and metabolic and immunological diseases.
Can fertility problems affect offspring?
Couples with fertility problems often have a slightly increased risk of having offspring with a disease or disability.
In cases where the cause of the fertility disorder is a chromosomal abnormality, a premutation of the FMR1 gene or a mutation in the cystic fibrosis gene, the risk of the child having a genetic disability may be increased. Therefore, it is very important to know the causes in order to take appropriate measures in the context of fertility treatment.
What are the objectives of these genetic studies?
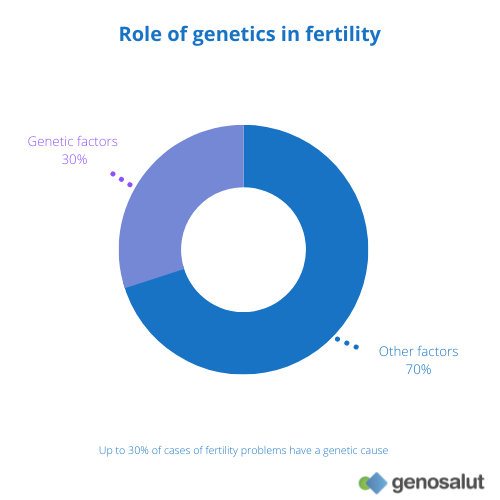
As mentioned, in up to 30% of cases fertility problems may have genetic causes. A genetic study can help determine the problem and dictate the steps to be taken.
The results of these genetic studies allow us to determine if there are:
- Problems that can be corrected.
- Irreversible problems that can be corrected by assisted reproduction techniques using the male’s sperm.
- Irreversible problems that cannot be corrected.
- Diseases that may be the underlying cause of infertility and require medical care.
- Genetic abnormalities that may be the cause of recurrent miscarriages or affect the health of the offspring (poor development and disabilities).
Who covers the costs of genetic diagnosis and counselling in cases of infertility?
As a general rule, genetic counselling is not covered by any kind of health insurance. Genetic testing for miscarriage or fertility problems is covered by some private insurance companies. You can come to us with a certificate from your doctor or with your insurance card.